

Introduction
An increased risk of mortality has been documented in transplanted patients affected by Coronavirus Disease 2019 (COVID19) with an estimated mortality rate between 20-40%. Multiple efforts are ongoing to control COVID19 pandemic, and clinical practice is being adapted at the same time as the pandemic progresses around the world. To reduce unnecessary in-person appointments has become crucial to minimize hospital exposition. Digital technologies allow us to perform real-time monitoring of patients' clinical status. A real-time patient monitoring system through the use of a smartphone application and wearable devices was implemented at our Center during the COVID19 pandemic.
Methods
Since March 2020, a real time patient monitoring system was implemented at our HCT program. All consecutive adults patients transplanted between April 2020 and July 2020 were considered for the study. Vital signs and relevant clinical information were reported during 14 consecutive days after being discharged, through the online platform provided by Trilema Fundation (saludencasa.trilema.org, Fundación Trilema, Valencia, Spain). Vital signs (cardiac frequency, blood pressure, oxygen saturation) were measured with validated oxymeters (Onyx II®, Nonin Inc, Plymouth MN USA) and blood pressure monitors (iHealth Track®, Mountain View, CA USA). Temperature was measured through domiciliary thermometers. Patients were educated to measure their respiratory frequency. A checklist of clinical symptoms was filled daily. An analogue visual scale (0-10) to detect potential cases of anxiety or depressive disorders was reported daily. Scores of >6 were evaluated by a psycho-oncologist through videoconference. All the data were reported to the online platform using a smartphone app compatible with iPhone and Android systems. A direct chat between patients and physician was available through the app. Clinical information was daily supervised by an experienced HCT hematologist. Clinical interventions were arranged if significant clinical abnormalities were documented. A hematologist with experience in HCT patients revised all the patients' data daily. Programmed alarms were set in case of any of the following situations: fever >38 oC; oxygen saturation <92%; tachicardia >125/bpm, hypotension (sytolic<90 mmHg, diastolic > 60 mmHg; altered mental status; persistent emesis or diarrhea). Patient´s satisfaction questionnaires were evaluated individually after finalizing the 14-days clinical monitoring.
Results
During the study period, 21 adults underwent HCT and 16 were s were eligible to be recruited into the study (80% feasibility) with team effort and without additional costs. Reasons for not being enrolled were: language incompatibility (1 patient), no consent (1 patient), not compatible smartphone (3 patients). Of the 16 enrolled patients, median age was 50 (range 22-70 years), 37% were female and 94% had lymphoid diseases. Thirty-eight percent of HCTs were autologous and 62% allogeneic.
Of the 16 enrolled patients, 25% were not able to adequately use the app due to inability in using smartphone applications. Of the remaining 12 patients, adherence in reporting study data (number of days reported of the planned 14 days study period) was as follows (average):
temperature 89%, oxygen saturation 90%, respiratory frequency 70%, cardiac frequency 85%, blood pressure 89%, symptoms reporting 65%, emotional distress 71%.
Automatic alarms were activated only 3 times: twice for the presence of clinical symptoms and once, for emotional distress. A videoconference with the psycho-oncologist was requested by one patient only. The chat service to communicate with hospital personnel was used in 4 patients. Data collected with the digital system helped the clinician to early recognize arterial hypertension (1 patient) and acute cutaneous GVHD grade 1 (1 patient).
Only two patients of the whole cohort were readmitted within 14 days from discharge due to grade 4 odynophagia due to HSV1/2 reactivation.
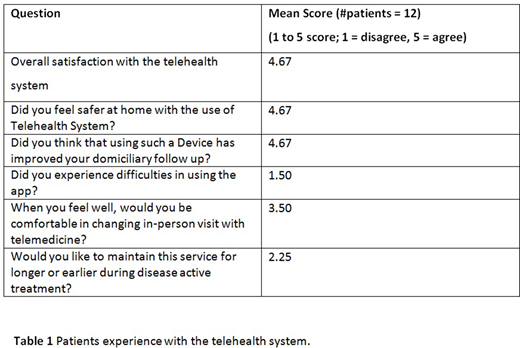
Patients´ experiences with telehealth systems are reported in table 1.
Conclusion
Telehealth monitoring can potentially improve patient's follow-up in terms of both physical and psychological outcomes. Technological problems still represent a barrier to a wider application of telehealth monitoring systems in the medical setting.
Mussetti:Novartis, Gilead: Honoraria, Research Funding. Sureda Balari:Incyte: Consultancy; Janssen: Consultancy, Honoraria; Celgene/Bristol-Myers Squibb: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; BMS: Speakers Bureau; Roche: Honoraria; Takeda: Consultancy, Honoraria, Speakers Bureau; Sanofi: Consultancy, Honoraria; Gilead/Kite: Consultancy, Honoraria; Merck Sharpe and Dohme: Consultancy, Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal